The Silent Saboteur: How Admin and Moral Injury Became the Twin Crises Driving Therapist Burnout.
Introduction
As an Executive MBA candidate, this consultancy project critically analyses a significant, yet under-researched, real-world challenge: burnout in private mental health therapists in the UK. While this topic may seem divergent from my primary clinical background as a haematologist, my decision is driven by a profound and relevant personal commitment.
Firstly, professional burnout is not abstract; as a clinician within an overstretched health service, I have personally experienced and witnessed the debilitating effects of systemic overload on accomplished colleagues. Secondly, I have immense gratitude for the therapeutic fraternity, whose crucial work has provided immeasurable benefit to people close to me.
This research, therefore, applies my academic and clinical rigour to amplify the voices of these vital practitioners. By leveraging quantitative analysis of survey data and qualitative exploration of experiences—particularly focusing on operational friction and moral injury—the project aims to deliver actionable, evidence-based solutions that can measurably lighten the load of the average therapist.
Literature review
Several previous studies have looked at this issue, not particularly from a UK or private practice perspective. A 2020 cross-sectional study of 298 qualified psychological therapists in the UK found a high prevalence of burnout (around 79% with high exhaustion and 58% with high disengagement). The quality of supervisory relationships was linked to lower burnout, suggesting that enhanced supervision could be a key burnout reduction strategy in UK therapists (including private sector therapists). [1] However, the participants in this survey were predominantly recruited from NHS organisations and there was little representation from private practice therapists. Another 2024 qualitative study on integrative psychotherapists highlighted the emotional challenges and burnout risks. Novice therapists experienced intensified burnout. Personal therapy, clinical supervision, and peer support were highlighted as crucial coping mechanisms. This study emphasized the need for structured support interventions in therapeutic professions.[2] A systematic review of 9 peer-reviewed studies specifically exploring psychological therapists’ experiences of burnout underscored severe professional and personal impacts of burnout. It emphasized the need for mixed-method research and burn-out management strategies tailored for psychological therapists. [3] Other studies from UK contexts highlight similar findings: high work demands, insufficient resources, poor management, and lack of support are core contributors to burnout. Newly qualified therapists report higher burnout due to workload stress and insufficient supervision. [4,5] NHS introduced a service called improving access to psychologic therapies (IAPT), now called NHS talking therapies. Dr Crystyn Scott studied burnout in staff working in IAPT as part of her doctoral thesis. She reported significant emotional exhaustion and stress linked to service demand pressures.
Taken together, the findings from these studies show that burnout is common in psychologic therapists, both private and public. Some studies have shown newly qualified therapists are particularly vulnerable and the quality of supervision is a key mitigating factor. The common causes of burnout include workload, resource scarcity, and management/administrative issues. Psychological therapists report that burnout not only affect their professional work and wellbeing, it percolates into their personal life too. Some suggested coping strategies include better supervision, peer support and better organisational and administrative support.
Methods
I contacted approximately 500 psychological therapists in private practice across the UK using email addresses publicly listed on a therapist directory (thepracticerooms.co.uk). Contact was made under the “legitimate interests” basis permitted within the UK GDPR framework for academic research outreach. No personal identifiable information was collected at any stage, and participation was entirely voluntary. As a token of appreciation, a £10 Amazon voucher was offered to the first 30 respondents. The questionnaire used in this research can be viewed here.
Want to remain updated about the latest activity here? Please leave you email.
Results
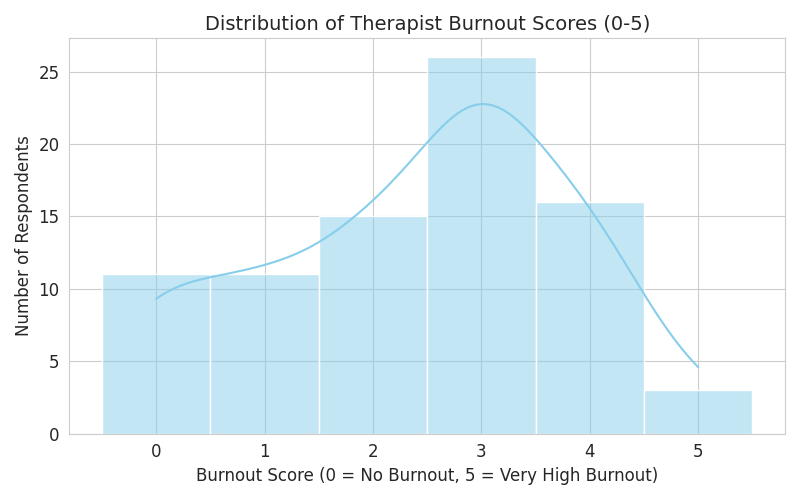
The survey included 82 respondents and used a Burnout Score from 0 (no burnout) to 5 (very high burnout).
Burnout Distribution and Severity
- Mean Burnout Score: The average reported burnout score was 2.41 out of 5.0, indicating a moderate-to-high level of collective burnout among the respondents.
- High Burnout Concentration: A significant portion of respondents reported a score of 3 or higher.
The distribution of burnout scores is visible in the chart below:
Correlations with Burnout
The analysis of how burnout relates to key professional factors yielded surprising results:
| Factor | Pearson Correlation with Burnout Score | Insight |
| Weekly Admin Hours | +0.25 | A positive correlation exists, suggesting that as time spent on non-client/admin tasks increases, the reported burnout score tends to increase. This is the strongest numerical correlate found. |
| Years of Experience | -0.07 | A negligible correlation. Burnout appears to be not strongly dependent on years of experience. |
| Weekly Client Load | -0.03 | A negligible correlation. Burnout appears to be not strongly dependent on the number of clients seen per week. |
This suggests that administrative burden is a more significant statistical driver of burnout than client volume or professional tenure.
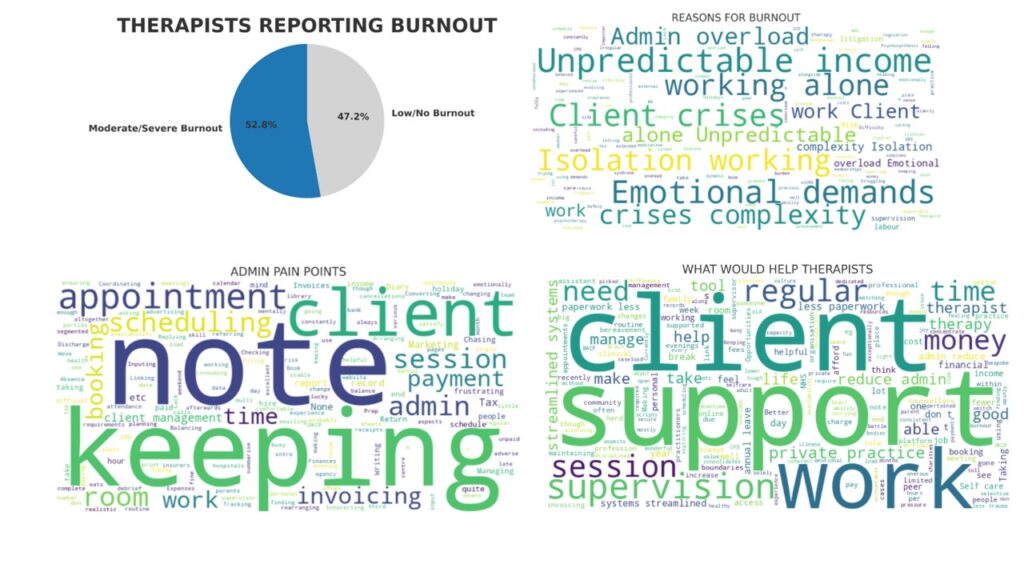
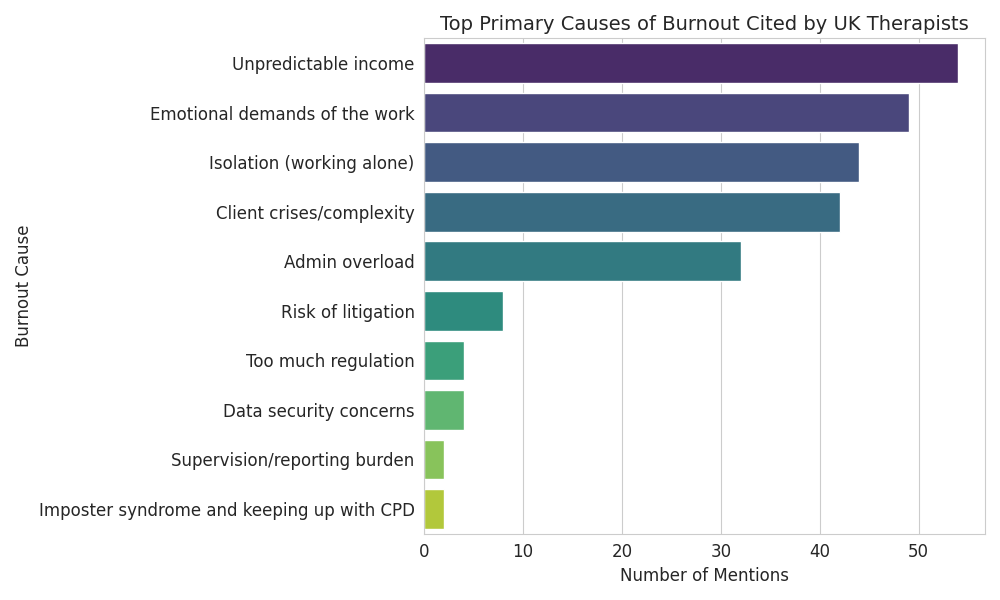
Primary Causes of Therapist Burnout
Respondents were asked to select all primary causes of burnout that apply. The top three causes cited are highly consistent:
- Emotional demands of the work: 70%
- Isolation (working alone): 63%
- Admin overload: 52%
The top causes are visualized in the chart below:
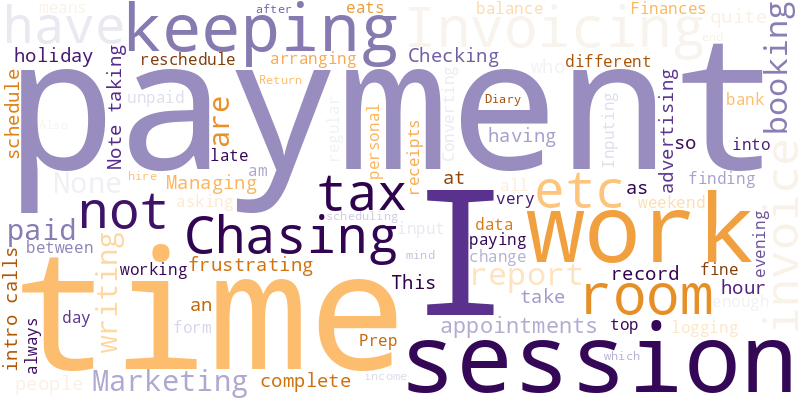
Administrative and Operational Pain Points
When asked about their biggest operational or admin pain point, the free-text responses frequently mentioned:
- Invoicing / Chasing payment
- Scheduling / Rearrangement of appointments
- The volume of emails
- Fragmented digital systems
The frequency of these terms is illustrated in the word cloud:
Solutions for Burnout Reduction
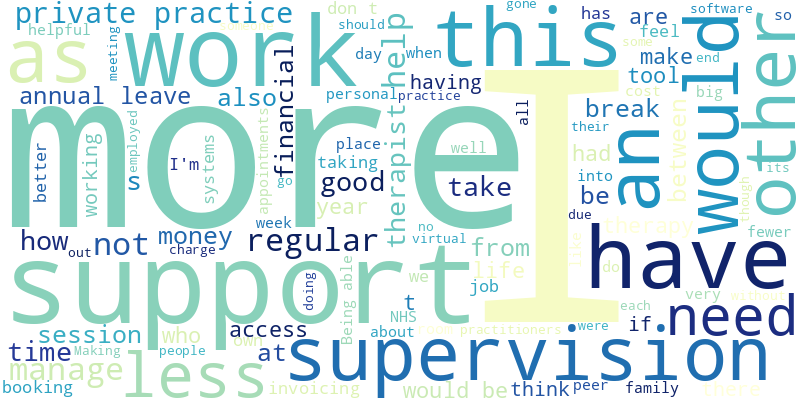
When asked what would most help reduce burnout, the free-text responses centered on themes of:
- Support: (e.g., PA, admin support, assistant)
- Money: (e.g., salaried, better pay, funding)
- Time/Flexibility: (e.g., fewer hours, more space)
The frequency of these terms is illustrated in the word cloud:
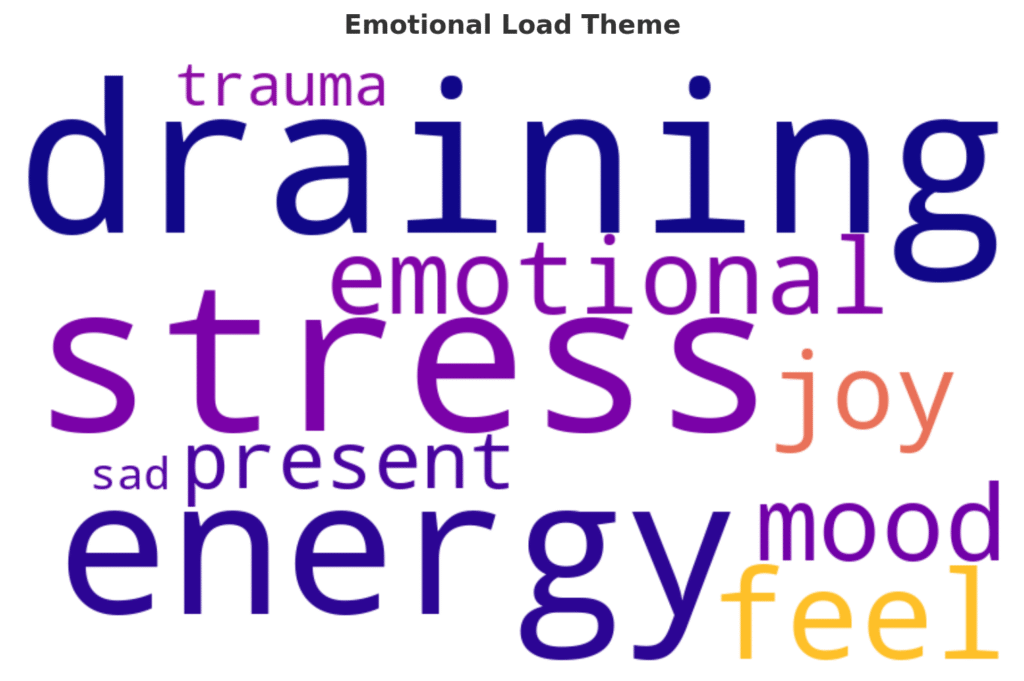
Top 3 Holistic Themes from this survey
I analysed the rich free text response and grouped them into three distinct themes.
- Emotional load
- Systemic/Business pressure
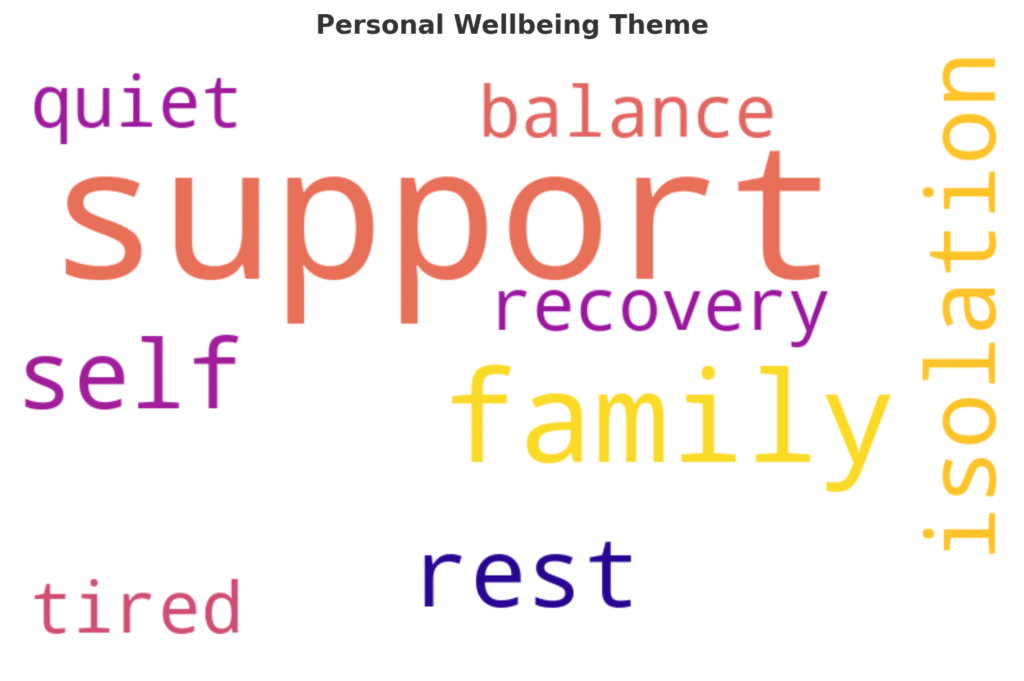
- Personal well being
The following word clouds capture the essence of these 3 themes.
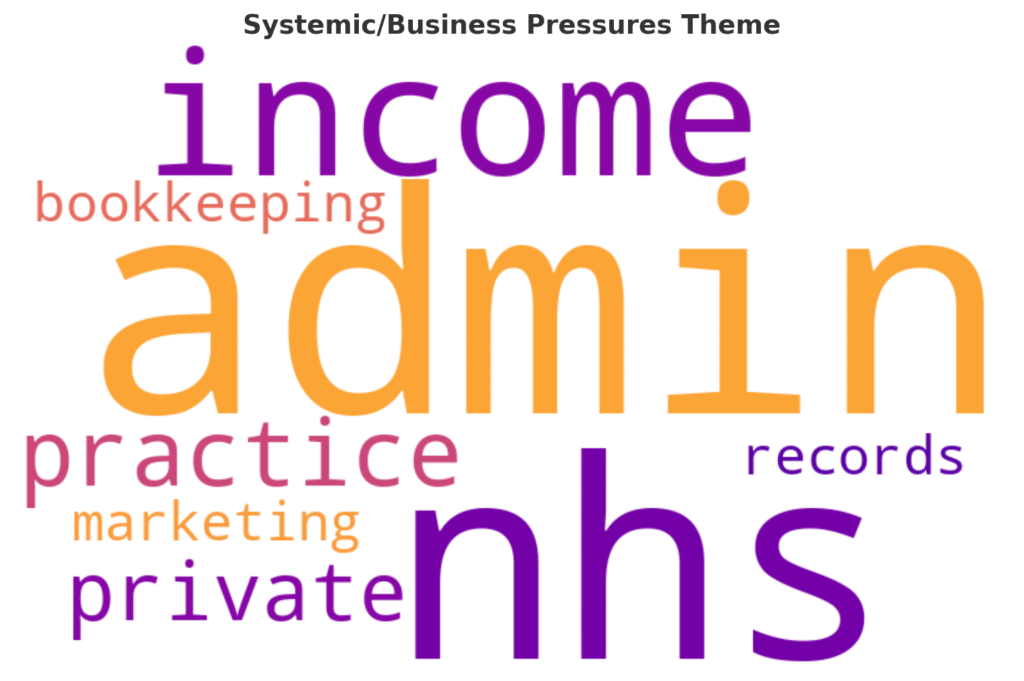
“Systemic/business Factors” highlight a crucial, non-numerical stressor: Moral Injury.
To me, this was the most overlooked factor. This reveals the therapist’s despair at not being able to help clients against external forces: poverty, housing crises, funding cuts, and the limitations of the NHS (“the system”). The pain is less about the client and more about the inability to fight social injustice. It’s not just the complexity of trauma that drains them, but the feeling of futility when they are aware that the client’s problems are caused or exacerbated by external forces (e.g., “The system is toxic,” “social inequality,” “capitalist reality”). This stress—knowing the solution is outside the therapeutic room—is a distinct and profound form of burnout not captured by the “Emotional Demands” category alone.
Want to remain updated about the latest activity here? Please leave you email.
Discussion
The findings of this survey confirm that UK mental health therapists experience a significant level of professional strain, with an average reported burnout score of 2.41 out of 5. While the emotional demands of therapeutic work are the most frequently cited cause of exhaustion, the correlational data suggests a more insidious driver: the administrative burden. The weak-to-moderate positive correlation between time spent on non-client tasks and a higher burnout score (r = 0.25) indicates that operational friction, rather than therapeutic intensity or client volume, is the most statistically relevant factor pushing practitioners toward exhaustion.
This section will discuss these results and propose targeted, practical solutions—both systemic and technological—to address the identified pain points.
The Problem of Operational Friction
The survey highlighted a clear ‘Admin Trifecta’ of pain points: Invoicing/Payment Management, Scheduling/Messaging, and Note-Taking. These tasks are high-frequency, repetitive, and interrupt the core therapeutic focus, forcing clinicians to operate simultaneously as small-business administrators. The requests for “PA support” and “salaried roles” indicate a deep, structural desire to delegate or eliminate the business infrastructure requirements of private practice.
Practical Solutions for Admin Pain Points
| Pain Point | Proposed Solution Category | Actionable Recommendation |
| Invoicing/Chasing Payment | Financial Automation | Mandatory Upfront Payment System: Implement systems that require payment details (card on file) and charge the client automatically before the session begins. The only subsequent action required should be a receipt delivery. Eliminate the concept of “chasing payment.” |
| Scheduling/Messaging | Client Self-Service & Integration | Unified Communication Platform: Utilise secure Practice Management Software (PMS) that integrates client messaging, scheduling, and calendar sync into one application. This should include automated intake forms and cancellation/reschedule fees, thereby minimizing therapist involvement in logistical triage. |
| Note-Taking / Paperwork | Efficiency & Delegation | Dictation/Speech-to-Text Integration: Implement GDPR-compliant tools that allow therapists to dictate notes immediately post-session, which are then securely transcribed and integrated into the client file, drastically cutting down on evening/weekend administrative creep. |
Addressing the Intrinsic Emotional Load
Despite the statistical focus on admin, the Emotional Demands of the Work remains the top reported cause of burnout. Furthermore, the free-text analysis revealed critical internal stressors: the chronic cognitive burden of containment and the pain of moral injury stemming from systemic limitations (poverty, social injustice). Addressing this intrinsic load requires structural support for the therapist’s internal world.
| Intrinsic Stressor | Proposed Solution Category | Actionable Recommendation |
| Containment Burden (Holding client distress) | Structured Decompression | Mandated Transition Time: Encourage the scheduling of at least 15-20 minutes of non-negotiable personal time between clients. This time is for grounding, not admin, allowing for psychic ‘discharge’ and full presence for the next client. |
| Isolation (Working Alone) | Community & Peer Support | Formalised Peer Consultation Groups: Move beyond traditional clinical supervision by creating structured, secure groups for emotional processing and case debriefing, focusing on the therapist’s reaction to the material, not just clinical strategy. |
| Moral Injury (Systemic Helplessness) | Advocacy & Validation | Professional Advocacy Channels: Establish a clear mechanism within professional bodies or platforms for therapists to report and aggregate the impact of social determinants (e.g., housing, poverty) on client mental health, legitimising the external source of pain and fostering collective advocacy. |
Entrepreneurial Focus: Building the Solution
For entrepreneurs looking to build impactful solutions for the therapist community, the focus must shift from merely building a generic software platform to creating a delegation ecosystem that specifically addresses the high-correlation burnout driver (admin time) and the high-frequency burnout driver (emotional load).
The following three pillars represent the most critical areas for entrepreneurial investment:
The ‘Invisible’ Financial Engine
A successful system must make money management invisible to the therapist. This means:
- Zero-Touch Invoicing: Automatic billing, integrated fee structures (including automated late-cancellation charges), and direct payment into the practitioner’s account with minimal reporting required.
- Income Security Features: Tools for predicting cash flow stability based on current bookings, directly addressing the stress of “Unpredictable Income,” the third-most cited cause of burnout.
The Delegated Communication Gateway
The system must act as a ‘Virtual Administrative Assistant’ for common, repetitive tasks:
- Automated Intake Funnel: Managing the initial “Initial contact” pain point by providing self-service booking, pre-qualifying screening questions, and secure document signing before the first contact with the therapist.
- Smart Scheduling Logic: Using AI or complex algorithms to manage the “juggling” of reschedules and cancellations according to predefined rules, notifying the client and updating the calendar without requiring therapist intervention.
Community, Containment, and Resilience
Given that Isolation (working alone) is the second-most common cause of burnout, the platform must integrate a professional community solution that also supports psychic containment:
- Integrated Peer Consultation & Decompression: A feature allowing secure, GDPR-compliant sharing of anonymized case notes or questions with verified peer networks within the platform, directly addressing the lack of immediate support. This module should also include tools for timed decompression breaks (e.g., guided breathing exercises or time tracking features to enforce the 15-20 minute transition time).
- Virtual Co-Working Spaces: Structured, time-limited virtual sessions where therapists can silently work on admin tasks alongside peers, fostering a sense of shared professional life without demanding active social interaction.
By focusing on these practical solutions—especially those that automate or delegate the “Admin Trifecta” and provide structure for emotional containment—entrepreneurs can build systems that reduce both the statistically strongest and the most frequently reported drivers of burnout, thereby allowing therapists to concentrate their energy on the emotional demands that require their unique human expertise.
About Me
I’m Dr. Sriram Ravichandran, a clinician, academic, and founder who believes technology should make human care more human, not less. I’m building HearMeNow to change that story.
I would like to expand this work by speaking to psychological therapists about their experience of burnout. I am organising weekly sessions that are just a space to speak and hear without any prejudice.
You can book a slot through this link- https://bit.ly/43Ryprt
References
[1] Johnson J, Corker C, O’Connor DB. Burnout in psychological therapists: A cross‐sectional study investigating the role of supervisory relationship quality. Clinical Psychologist. 2020;24(3):223-235.
[2] Tragantzopoulou P, Giannouli V, Filippou A, et al. Burnout and Coping Strategies in Integrative Psychotherapists: Findings from Qualitative Interviews. Healthcare. 2024;12(18):1820.
[3] Vivolo M, Owen, J., & Fisher, P. Psychological therapists’ experiences of burnout: A qualitative systematic review and meta-synthesis. Mental Health and Prevention. 2024;33.
[4] Davies S, A Sriskandarajah S, A Staneva A, et al. Factors influencing ‘burn-out’ in newly qualified counsellors and psychotherapists: A cross-cultural, critical review of the literature. Counselling and Psychotherapy Research. 2021.
[5] Klingemann JI, Wieczorek Ł. A crisis of exhaustion in the game of escalation: a qualitative exploration of the consequences of occupational burnout among addiction therapists. Postep Psychiatr Neurol. 2024;33(1):18-25.